Imagine that you decided to temporarily shut down your business. You made this decision because you knew something major could go wrong and, despite some efforts, you didn’t make as much progress as you hoped. So, you temporarily closed without knowing how long “temporarily” would be.
Three months later, you have made big changes. Massive, ginormous, monumental changes. Changes to foundational elements of your business. You discontinued a beloved product, made existing products safer and expanded a controversial product.
Now, imagine that the press followed all of this. They reported on every meeting, speculated on every discussion, and critiqued every statement. They even said you should be fired.
But now, today, you announced that you’re open for business. All the problems are solved, and all the changes rolled out. The press celebrated, and articles, podcasts, and news stories heralded your business’ re-opening.
Your customers yawned.
They didn’t miss you.
Many didn’t even know you were gone.
A True Story
You just read the story of Major League Baseball at the end of its 99-day lockout.
But it could also be the story of your business if you make the same mistake MLB did in December, which is the same mistake it has made for the past 20+ years.
It forgot what business it’s in.
MLB thinks it’s in the baseball business. For some customers, diehard fans, it is. But for most, baseball is in the business of helping customers to:
Make memories
Have fun
Feel connected to others
Be entertained
Drink beer and eat junk food without guilt
These are the Jobs to be Done that customers hire baseball to do for them. But there are dozens of other businesses offering to do the same Jobs, many in ways that are lower cost and more easily accessible. And fans are taking their business to those competitors.
According to Statista, the average per game attendance was 18,900 in 2021, a 34% decline from 2019. Even more troubling than this “generational low” is that people aren’t even watching baseball at home, evidenced by the 12% decline in TV viewership for games.
Customers are rejecting baseball. They just don’t care about it as much as they used to. As a result, they’re spending less time and less money on it and finding newer and better alternatives.
3 Questions to Figure Out if You’re Out (or In)
This story isn’t unique to MLB. It’s the story at the core of many failed businesses. The outward view of solving customers’ problems gives way to an increasingly inward-facing view of the business the business is in.
The story isn’t fast-paced or obvious, either. The declines happen slowly – average gameday attendance dropped only 367 people annually from 2012 to 2019, a decrease that’s easy to miss when considering that the average MLB ballpark holds 43,000 people.
But once the decline starts and apathy sets in, it is challenging to change the story. But not impossible.
If you want customers to care about you again, to need you and your products the way they used to, you need to care more about your customers than your business. You need to ask three questions:
1. “Why do you choose us?” (in Innovation-speak this translates to, “What are your Jobs to be Done?”)
2. “When you don’t choose us, who do you choose and why?”
Then you must listen. Really listen. To EVERYTHING customers say. The reasons you want to hear and the ones you don’t, The competitors you know and the ones you least expect. The things that make them better that you know and the ones you don’t agree with.
Then, and only then, do you look inward at your operations and business model and ask.
3. “What business are we in?”
Are your operations set up to deliver delight to customers or maximum efficiency to your business? Is your business model set up to create value for customers or maximize profit for you? Are you increasing the size of bases 3 inches and claiming its safer or doing everything possible to reduce the game’s length and increase its fun factor?
It’s not customer rejection that kills a business. It’s customer apathy.
Don’t allow your customers to become apathetic. They cared about your business once. Keep giving them reasons to care by asking what they care about and delivering it.
How do you make sure that you’re in the right business?
When you were a child, you knew that the best stories began with “Once Upon a Time” and end with “And they lived happily ever after.” As an adult, you know that stories can begin and end any number of ways.
As a leader trying to grow a business, it may seem like all your innovation stories end with “And then we cancelled the project/disbanded the team/got distracted by the needs of our current business”
Why is that?
How can you change your innovation story the endings to “And they lived happily ever after (because they launched lots of cool new stuff that people loved and paid for and that led to new revenue and lots of growth and happy employees and other wonderful happy things)”
While there are hundreds, if not thousands, of answers to those questions, one of them is in the way you start the story.
How the story begins
Think about the last time you kicked off an innovation project. What did you say?
Story 1: “We need you to work on X and we don’t want you to be encumbered by what we’ve done in the past. We want you to explore, think creatively, and really push our thinking.
Story 2: “We need you to work on X and, to save you time, here is everything we did in the past. Use this as a starting point and build from here.
Story 3: We need you to work on X. Here’s what we did in the past, but we’re not tied to it. Look it over and let me know what you think we should do from here.
There’s nothing obviously wrong with any of these.
Just like “Once upon a time,” they start with clear direction – we need you to work on X. Even better, they all express your positive intentions and support (push our thinking, save you time, let me know what you think) for the team.
What could possibly go wrong?
How the story ends
The team returns from their quest, which usually involves a lot of research, to present their findings and recommendations. They are excited by what they discovered and eager to continue their work. They conclude their presentation and turn to you, eagerly awaiting your response.
If you started with #1
Thinking of all the freedom you gave at kickoff, and sigh. “That’s good work but we already knew most of that. We wanted you to push our thinking, but I don’t see a lot of new here.”
The team nods and tries to point out the new insights but to no avail. The gather their things and walk out. At best they feel dejected, like they failed an important test. At worst, they’re angry, feeling like the whole exercise was a trap. They know you’re disappointed and, as a result, the end is near.
If you started with #2
Thinking back to the dozens of files you gave them at kick-off, you lean forward and say, “That’s good work but we already knew most of that. To be fair, you built on what we had but why did it take so long?”
The team looks at each other, trying to hide their confusion. They built on what you gave them and delivered it on time. Not knowing quite what to say, they gather their things and walk out. Frustrated, they feel like they were set up to fail. After all, why would you give them so much time if you didn’t want them to use it? They know you’re frustrated too and brace themselves for the repercussions.
If you started with #3
You think back not to the kickoff but to the meeting after that, the one where the team presented their research plan. You take a deep breath and say, “That’s good work but we already knew most of that. To be fair, you did warn me that might be the case. I can see where some things shifted and where we gained new insights.”
The team nods and lays out the implications of their findings. They layout the milestones between today and a potential launch, and detail next steps to hit the next milestone. As before, you debate the insights and the plan, ultimately coming to agreement on what happens next. The team gathers their things and leaves the room, motivated to continue their work
What went wrong?
Three stories began but only 1 is on track for a “happily ever after.” The first two stories began with such promise, but they ended with dejection, anger, disappointment, confusion, and frustration. Why?
Unrealistic expectations
If you started with #1, you set unrealistic expectations. As a leader in the organization, you know more about the business than the team so it’s not realistic to expect the team to tell you something you don’t know. As someone with years of experience in the industry, you know that things don’t change overnight so even research that’s a few years old is still probably more right than wrong. Expecting the team to “push your thinking” and tell you something you don’t know isn’t realistic. Worse, it’s not fair.
Orders, not ownership
If you started with #2, you made it very clear from the start that you’re the expert by telling the team to take past work as a given and build on it rather than question it. You probably also gave them a timeline and told them to come back to you at the next milestone. You did all this to help the team work efficiently and you wanted them to feel ownership, to question the work and take the time they need, even if it’s less than the time given. But the team did exactly what you asked because you gave them orders and, in most companies, success comes from following orders.
What went right?
What did you do in #3 that put the team on path to “happily ever after?”
You were honest and transparent about past work. By sharing past work, you made it clear that you trusted the team to think critically and creatively, to analyze past data and make decisions about what should be kept, questioned, and discarded.
You invited the team to challenge you. When you shared the past work, you gave the team insight into your current hypotheses and biases. By admitting that you’re not tied to past work, you made it clear to the team that you were open to discussion and willing to change your mind.
You empowered the team to take ownership. By asking the team to review past work then come back to you with suggestions and plan, you gave them ownership of the process. When they left that first meeting, they were responsible for the work AND how the work got down. They were project owners now
The End (almost)
Good intentions aren’t enough to set innovation projects and teams up for success. How you start the story by setting expectations and empowering the team has a huge impact on how the story progresses and whether or not it ends “happily ever after.”
In Part 1, you learned the What, Why, and How of 5 popular Innovation Frameworks – Human-Centered Design (also known as Design Thinking), Systemic Design, User-Centered Design, Lean Start-up, and Agile.
But as anyone who grew up in the 1980s and watched G.I. Joe will tell you, knowing is half the battle.
The other half is doing. More specifically, doing the right thing at the right time.
This brings us to Part 2 – the When of our 5 Innovation frameworks.
The Innovation Process
Before we get into the specifics of when to use each framework, let’s get clear on the activities that need to happen and the order in which they need to happen. In other words, we need to define an Innovation Process.
I know that sounds like an oxymoron. After all, you know that innovation is not a linear process. At best, it’s iterative. Usually, it looks and feels like this:
But you also know that this image doesn’t inspire confidence in senior leaders because it looks like chaos and doesn’t haven’t a timescale.
So to make the process more palatable to the powers that be, the Innovation Process is often shown as linear. Something like this:
Of course, that means that we, the innovators, must explain that the work isn’t, it’s an infinite loop with exit points at each step, and not every project can or should complete all the steps. It’s not perfect, but it serves its purpose (reassure senior leaders that we have a plan), so we’ll use it to help guide us to when to use each Innovation Framework.
Frameworks in the process
Now that we know the basic order in which activities should occur, we can return to our frameworks to determine which ones will best serve us in each step of the process.
“But wait!” some of you may exclaim. “Can’t we use them all?”
You can, but you don’t need to. Human-Centered Design and User-Centered Design are incredibly similar, and trying to use them both is more likely to confuse than clarify the work to be done.
“I knew it!” others will laugh, “that’s why I only use (fill in the framework).”
You can, but you shouldn’t. Every innovation has its strengths and weaknesses. The most successful innovators pull the best approaches and tools from each framework into their process.
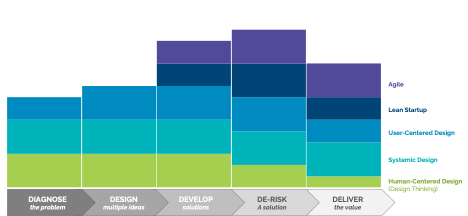
Here’s how I think things fit together:
How to Interpret: The thicker the colored band in a column, the better suited the Innovation Framework is for the phase in the process. For example, Human-Centered Design is excellent for Diagnose, Design, and Develop phases, useful in De-Risk, and ok in Deliver. In contrast, Agile is not at all suited for Diagnose and Design but is excellent for De-Risk and Deliver.
In Diagnose and Design, lean heavily on Human-Centered Design because it keeps you open to all the types of people involved in the problem and the solution (not just users). If you’re operating in a complex environment, like healthcare or education, being in Systemic Thinking to make sure you don’t miss non-human elements like regulation, technology, or geopolitical dynamics that could also have a significant effect on the problem and eventual solution
In Develop, start weaving in elements of Lean Startup, especially its focus on building business models and not just individual products or services. Tools like the Business Model Canvas are a huge help here and reveal critical but non-product/service assumptions that need to be tested.
In De-Risk, Lean Startup and Agile become (relatively) interchangeable, so use the language that best resonates within your organization. The key here is to apply the Scientific Method to your solution through rapid prototyping and testing.
In Deliver, you’ve launched your solution, and the goal is to scale. Agile is designed for this, but it’s essential to keep the human/user at the center of continuous improvement efforts.
Popular “Innovation” Frameworks: Now What?
You’re now even more of an expert on five popular innovation frameworks, ready to talk the talk and walk the walk with the best of ’em. Right?
Maybe.
This is all the opinion of one person in a world of experts who think and who do. So what did I miss? What did I get wrong? Drop a comment, and you’ll make us all smarter!
Click here to automatically download the What, Why, How, and When Cheat Sheet
Forget secret handshakes, guarded rituals, and clandestine meetings. The easiest way to show that you’re a part of the “In-Crowd” is by throwing around obscure terms and incomprehensible acronyms.
Every industry has words and acronyms that only make sense to insiders. Stock traders have BOP (Balance of Power), Consumer Goods companies have ACV (All Commodities Volume), and, thanks to the military, we all have SNAFU (Situation Normal: All F-cked Up)
Innovators are no different. We throw around terms like Design Thinking, Lean Startup, ethnography, Discovery Driven Planning. We rattle off acronyms like VUCA JTBD, and MVP.
But do we really know what the industry terms and acronyms mean?
More importantly, are we sure that our definition is the same as our boss’ or colleague’s definition?
If you’re even a little bit like me, your answer to both of those questions is No.
And that feels awkward because it can lead to confusion, frustration, and disappointment in your work and your team.
So, let’s get back on the path to building clarity, efficiency, and support in your innovation efforts!
In Part 1, we’ll get into the What, Why, and How of the 5 of the most popular Innovation frameworks. Next week, in Part 2, we’ll dig into the When of each framework in the innovation process.
Popular “Innovation” Frameworks: What, Why, and How
What it is: A problem-solving framework that integrates the needs of people, the possibilities of technology, and the requirements for business success grounded in 3 principles:
Inspiration: Understand customer needs
Ideation: Generate creative ideas
Iteration: Rapidly prototype and test
Why it is important: Useful in solving “wicked problems,” problems that are ill-defined or tricky and for which pre-existing rules and domain knowledge will be of limited or no help (or potentially detrimental)
How you do it:
Qualitative research with tools like ethnography and Jobs to be Done to build empathy with the customer
Ideation to identify and explore lots of possible solutions
What it is: A way of making sense of the world’s complexity by looking at it in terms of wholes and relationships rather than by splitting it down into its parts; grounded in 5 principles:
Acknowledge the interrelatedness of problems
Develop empathy with the system
Strengthen human relationships to enable creativity and learning
Influence mental models to facilitate change
Adopt an evolutionary design approach to desired systemic change.
Why it is important: The increased complexity caused by globalization, migration, sustainability renders traditional design methods insufficient and increases the risk that designs result in unintended side effects.
How you do it:This is an emerging innovation discipline with multiple schools of thought and dozens of potential tools. To learn more and find tools, check out the Systemic Design Association.
What it is: A framework in which usability goals, user characteristics, environment, tasks, and workflow of a product, service, or process are given extensive attention at each stage of the design process and grounded in 6 principles
Design is based upon an explicit understanding of users, tasks and environments.
Users are involved throughout design and development.
Design is driven and refined by user-centered evaluation.
Process is iterative.
Design addresses the whole user experience.
Design team includes multidisciplinary skills and perspectives.
Why it is important: Optimizes the product around how users can, want, or need to use it so that users are not forced to change their behaviors and expectations to accommodate the product.
How you do it:Personas, scenarios, and use cases that capture the context, behaviors, habits, and instincts with
What it is: A methodology for developing businesses and products that emphasizes customer feedback over intuition and flexibility over planning, grounded in 5 principles:
Entrepreneurs are everywhere.
Entrepreneurship is management.
Validated learning.
Innovation Accounting.
Build-Measure-Learn
Why it is important: Aims to shorten product development cycles and rapidly discover if a proposed business model is viable
What it is: A project management philosophy that expanded to be used in innovation and business transformation
Individuals and Interactions Over Processes and Tools
Working Software Over Comprehensive Documentation
Customer Collaboration Over Contract Negotiation
Responding to Change Over Following a Plan
Why it is important: Improves time to market, quality, and employee morale
How you do it:The most common tools are:
Agile teams that are small, entrepreneurial, and empowered groups
Operating Model with focuses on leadership and culture, management systems, structures, talent, and processes
So What?
By now, you’ve probably noticed that the frameworks above are very similar – many of them are centered on the customer, value diverse experience expertise when creating solutions, and prioritize iteration over perfection.
So, which should you use?
The answer to that question depends on two things: your company and where you are in the innovation process. We’ll dive into those topics next week.
As you wait patiently for Part 2:
Tell me what I got wrong, what I missed, and what you think in the comments
Download this handy cheat sheet to the What, Why, and How of 5 Popular Innovation Frameworks
Before setting off on a journey to strange lands, most travelers take time to learn an essential phrase or two in the native tongue. After all, the ability to say “Hello” or “Help” or “Where’s the bathroom?” in the local language can mean the difference between a trip you remember forever and one that you want to forget immediately.
The same is true for people in large companies who set off on a quest to innovate – you’re in a strange land, and having a few handy phrases at the tip of your tongue can mean the difference between success and failure.
Here are the four most important phrases you should know as a corporate innovator
What does success look like?
Ask this at the beginning of every innovation effort. If you don’t, it’s very likely that what you view as success and what decision-makers view as success will be two different things.
Staffing up a new innovation team? What does success look like?
Starting a new project? What does success look like?
Developing and testing a prototype? What does success look like?
And don’t accept a vague or even qualitative answer to the question, like “we’ll know it when we see it” or “better employee engagement.” You need to know precisely what an effort contributes to and how leaders will evaluate the effort. Otherwise, it’s easy for managers to “move the goalposts” right when you think you’re about to score.
We expect a new innovation team to hold five brainstorming sessions and test 3 new products this year
We need this project to generate $10M revenue in 3 years from today
We need to understand how consumers will use this if we don’t give them any directions
Will you help me?
This question is perhaps the most challenging but most potent phrase in the innovation-to-corporate dictionary.
By the very nature of your work – making something new that creates value – you’re doing something that doesn’t fit cleanly into the existing structure. While that can be liberating, it also means that there are few, if any, people obligated to give you advice, resources, or support. That’s where this phrase comes in.
We all love to feel important and valued, and nothing makes people feel more important or valued than being asked for help. Plus, when you ask for help, people feel like they’re contributing to what you’re doing and start to feel a bit of ownership (or at least fondness) for it. Soon, you not only have advisors, but you also have partners, advocates, and champions.
Tell me more
This phrase is the ultimate innovation jiu-jitsu phrase because it turns your opponents’ strength (of opinion) against them and gives you powerful insights.
That will never work. Intriguing, tell me more.
We tried it, and it failed; the same thing will happen this time. I didn’t know that, tell me more.
If you do that, you’ll be fired. We don’t want that, so tell me more about why that would result.
Sometimes the rationale behind powerfully delivered dogmatic statements is logical and valid. Often, it’s emotional. The person who said it would never work is afraid that, if it does, their job will be in jeopardy. The person who remembers when it was tried before still bears the scars of that attempt and wants to protect you from the same experience. The person who says you’ll be fired for doing something may think that the rules are stricter than they are, and they’re trying to help you.
This phrase helps you figure out the reason behind the statement, the Why behind the What, so you can figure out what is true versus believed and how to get to your desired outcome.
What do you need to see to say “Yes”?
This question is my personal favorite, taught to me by a good friend, career innovator, and successful entrepreneur.
It is easy to say “No” and, in fact, that is the purpose of many people in a large organization.
Legal says No to keep the company o the right side of the law and out of lawsuits.
Accounting says No to keep the company financially healthy
Your boss says no because you have more work than you can handle, and this doesn’t seem essential.
Sometimes “No” is the correct answer. But if you start there, you’ll never know if it is the right answer or just the first, easiest, or most instinctual answer.
So, once you hear “No,” engage the person you’re talking to in a quick intellectual exercise and ask what they need to see to say “Yes.” By engaging them as an expert and your thought partner, you’re lowering their defenses and bringing them into a problem-solving mindset. Plus, you’re getting valuable insight into the type of data and evidence required to make progress.
What are other phrases every innovator should know?
As anyone who has ever tried to quickly learn a language for an extended trip, you’re best served by seeking out multiple sources.
After all, if I relied solely on Rosetta Stone to learn Danish before I moved to Copenhagen, I would have arrived knowing only how to say “the girl is on top of the airplane” (phonetically, it’s “pia pa flu-va-ma-skine”) and not “Hello” or “Help” or “Where’s the bathroom?”
So what are the phrases you repeatedly use to navigate your corporate innovation journey?