
by Robyn Bolton | Jun 3, 2020 | Innovation, Tips, Tricks, & Tools
Last week, I published a post with a very simple goal – define innovation so we can stop debating what it means and start doing it.
The response was amazing. So, I figured that this week I would tackle another buzzword – Design thinking.
We’ve all heard it and we’ve probably all said it but, like “innovation’ we probably all have a different definition for it. In fact, in the last few months alone I’ve heard it used as a synonym for brainstorming, for customer interviews, and for sketching while talking. Those things are all part of Design thinking but they aren’t the entirety of Design thinking.
What I tell my clients
When a client asks if we’re “doing Design thinking,” here’s what I say;
“Yes, because Design thinking is a way of solving problems that puts customers and stakeholders, not your organization, at the center of the process and seeks to produce solutions that create, capture, and deliver value to your customers, stakeholders, and your company.”
The Basics
- What: One could consider the official definition of Design thinking to come from Tim Brown, Executive Char of IDEO, who stated that “Design Thinking is a human-centered approach to innovation that draws from the designer’s toolkit to integrate the needs of people, the possibilities of technology, and the requirements for business success”
- Why: Useful in solving “wicked problems,” problems that are ill-defined or tricky and for which pre-existing rules and domain knowledge will be of limited or no help (or potentially detrimental)
- How:
- Inspiration: Understand the problem by building empathy with stakeholders (deeply understand their functional, emotional, and social Jobs to be Done) and document that understanding in a brief that outlines goals (ideal end state), bounds (elements to be avoided), and benchmarks against which progress can be measured
- Ideation: Generate ideas using brainstorming to develop a vast quantity of ideas (divergent thinking) and then home in on the ideas at the intersection of desirability, feasibility, and viability that best fit the brief (convergent thinking)
- Implementation: Prototype ideas so that they can be tested, evaluated, iterated, and refined in partnership with customers and stakeholders, ensuring that humans remain at the center of the process.
- When: At the start of any R&D or development process
- Traditionally, design was involved only in the late stages of development work, primarily to improve a solution’s functionality or aesthetic. Design Thinking’s ability to pull the designer mindset into the earliest phases of development is, perhaps, one of the biggest impacts it has made on business and technical fields
- Where: Can be done anywhere BUT, because it is a human-centered approach, it must involve multiple human beings through the process
- Who: Anyone who is willing to adopt a “beginner’s mind,” an attitude of openness to new possibilities, curiosity about the problem and the people with it, and humility to be surprised and even wrong
Important Points & Fun Facts
- Design Thinking IS a human-centered design approach. This means that it seeks to develop solutions to problems by involving the human perspective at every single step of the process
- Design thinking is NOT synonymous with user-centered design though user-centered design could be considered a subset of Design Thinking because it gives attention to usability goals and the user experience
- Design Thinking was NOT invented by IDEO, but I would argue that they have done more to popularize it and bring it into the mainstream, especially into business management practices, than any other person or firm.
- Design Thinking IS the product of 50+ years of academic and practical study and application. Here’s some fun facts:
- 1935: The practice of Design thinking was first established by John Dewey as the melding of aesthetics and engineering principles
- 1959: The term “Design thinking” was coined by John E. Arnold in his book Creative Engineering
- 1991: the first symposium on Design Thinking was held at Delft University in the Netherlands
- 2000s: Design thinking is widely adopted as an innovation approach thanks to books by Richard Florida (2002), Daniel Pink (2006), Roger Martin (2007), Tim Brown (2009), and Thomas Lockwood (2010)
- 2005: Stanford’s d.school begins teaching Design thinking as a general approach to innovation
- Design Thinking is NOT just for radical/breakthrough/disruptive innovation
- Design Thinking IS useful for all types of innovation (something different that creates value) resulting from wicked problems. In fact, as far back as 1959, John E. Arnold identified four types of innovation that could benefit from a Design thinking approach:
- Novel functionality, i.e. solutions that satisfy a novel need or solutions that satisfy an old need in an entirely new way
- Higher performance levels of a solution
- Lower production costs
- Increased salability
If you want to learn more…
As noted above, there are lots of resources available to those who are deeply curious about Design thinking. I recommend starting with Tim Brown’s 2008 HBR article, Design Thinking, and then diving into IDEO’s extremely helpful and beautifully designed website dedicated entirely to Design thinking.
Here’s what I’d like to learn…
- Was this helpful in clarifying what Design Thinking is?
- What, if anything, surprised you?
- What else would you like to know?
Drop your thoughts in the comments or shoot me an email at robyn@milezero.io

by Robyn Bolton | May 27, 2020 | Innovation
When I worked on P&G’s WalMart sales team, one of my bosses was a big guy with an even bigger personality. He shared his opinions loudly and broadly and one of his opinions was that we needed to stop using the word “breakthrough.”
“If I have to hear one more time about some new ‘breakthrough’ soap, I will throw you out of this office myself!” he would bellow.
Years later, I can’t help but wonder what he would think of the word “innovation.”
In May 2012, The Wall Street Journal published an article positing that, as the word “innovation” increased in usage, it decreased in meaning. The accompanying infographic said it all:
- 33,528: Times “innovation” was mentioned in quarterly and annual reports in the previous year
- 255: Books published in the last 90 days with “innovation” in the title
- 43%: Executive who say that their company has a Chief Innovation Officer or similar role
- 28%: Business schools with “innovation,” “innovate,” or “innovative” in their mission statements
That may seem like a lot but, remember, that data is nearly 8 YEARS OLD!
The desire for and investment in Innovation in all its forms – accelerators, incubators, startup/venture studios, corporate venture capital teams – has only grown since 2012.
While this may seem like a good thing, the fact that the success rate of innovations hasn’t changed, means that most people react to “innovation” the same way my boss reacted to “breakthrough” – if you bring it up, they throw you out.
To avoid getting thrown out of offices, one of the first thing I do with my clients when we begin working to build innovation into an enduring capability within their companies, is re-establish what innovation is and is not.
Innovation IS something different that creates value.
When people hear the term “innovation,” they tend to think of new-to-the-world gadgets that fundamentally change how we live our lives. Yes AND it’s many other things, too. Let’s break down the definition:
- “Something” includes products and technology, it also includes services, processes, revenue models, and loads of other things. Consider this, many would argue, quite convincingly, that the Toyota Production System was one of the biggest innovations of the 20th century
- “Different” often surprises people. After all, even Merriam Webster defines innovation as “something new.” But here’s the thing, one of the most commonly cited innovations, the iPhone, wasn’t “new.” Even Steve Jobs admitted it when he said, in his keynote speech, that Apple was introducing three products – a widescreen iPod with touch controls, a mobile phone, and an internet connected device. The iPhone was, however, different because it combined those three devices into one.
- “Creates value” is probably the most important part of the definition. All innovations solve problems. Solving problems creates value. If you solve a big problem, either because it’s a problem lots of people have or it’s a very painful problem a few people have or something in-between, you create a lot of value for others and for yourself.
Innovation IS NOT a one-size-fits-all term.
Think of it this way, both a Kia and a Maserati are cars, but you wouldn’t expect to pay Kia’s price tag and get a Maserati (and vice versa). Similarly, both a convertible and a pick-up truck are automobiles, but you wouldn’t use your convertible to carry building equipment to a construction site.
With a definition as broad as the one above, it’s possible for “innovation’ to become even more meaningless as it gets applied to more things. That’s why it’s important to identify different types of innovation.
There’s no universally accepted set of innovation types, which is why I recommend companies consider defining at least three types that reflect their business and forward-looking strategies.
One of the most common set of innovation categories is based on the degree of change required for implementation:
- Core Innovation requires minimal or no change to the current business model (customers, offerings, revenue model, resources and processes). Also known as Continuous or Incremental Innovation, this is the unglamorous but deeply important work of constantly improving what you do and how you do it.
- Adjacent Innovation changes a significant change to at least one element of your business model. It could be changing who you serve, like expanding from interventional cardiologists to general cardiologists, what you offer, like P&G’s expansion into “durable goods” when it launched Swiffer, or how you offer or deliver it.
- Radical innovation is the stuff that gets all the press. These innovations fundamentally change the business, like IBM moving from computers to business services. These innovations are high-risk and require a lot of time, money, and patience to see to fruition. This type of innovation is also called “Breakthrough” but, for obvious reasons, I shy away from that term.
There are many things that need to be done to shift innovation from buzzword to business capability. Defining innovation AND at least three different types is only the first step in moving from innovation theory and theater to building innovation into a true capability that drives sustainable growth.
Or, as I would tell my old boss, “It’s the first step. But it’s a breakthrough one.”
Originally published on December 30, 2019 on Forbes.com

by Robyn Bolton | May 13, 2020 | Customer Centricity, Innovation, Stories & Examples, Strategy
I took my last flight on Friday, March 13, two days after the president’s first address to the nation about COVID-19.
It was a JetBlue flight from Charlotte, NC back home to Boston. And it was awesome!
Setting aside the fact that I was wearing disposable gloves and wiping down every surface with Clorox wipes, I felt like I was flying private. I was the only person in my row, with no one in the row ahead of or behind me. Snacks and drinks were plentiful. The stewards were friendly and attentive. Even the boarding process was swift and orderly.
But when stay-at-home orders went into effect the following Monday and I shared my travel story with clients, they were aghast. How could I take such risks? Did I feel safe? Did I wear a mask?
Their reactions surprised me. After all, these executives are frequent travelers, even road warriors they travel so much. Yet the fear in their voices revealed a changing perception of travel. What was once a necessary evil for work and an efficient solution for vacation had, in just 3 days, become a senseless risk.
In the 2 months since that flight, the airline industry has been rocked. Consider:
- 94% drop in US commercial airlines’ passenger volume
- 80% decrease in US private jet flights
- 75% decrease in the number of worldwide commercial flights per day
- 80% decline in the global daily number of flight searches
- 61% increase in the amount of time between booking and traveling
That last stat – 61% increase in the amount of time between booking and traveling – indicates that people don’t expect to fly any time soon. But is that expectation a reaction to the drastic measures taken to flatten the curve or is it a sign of changing travel habits?
Many experts and industry associations are looking to data about the airline industry’s recovery post-9/11 and the 2008 global financial crisis. According to data from Airlines for America, it took 3 years for passenger volume and revenue to return to pre-9/11 levels and approximately 7 years to recover to pre-2008 financial crisis levels.
Here’s the harsh truth – we cannot possibly know what will happen next. 9/11 and the 2008 financial crisis were fundamentally different events than what we’re experiencing now.
So while I understand why people are looking to these past events – data offers a sense of comfort and control over the future – using data from them is pointless. It offers a warm snuggly illusion that things won’t change that much and a return to the old days is inevitable.
Instead of looking to the past for answers, we need to look to physics.
Newton’s 3rd Law, to be precise. It states that for every action, there is an equal and opposite reaction.
By looking at the actions that airlines, and regulatory and legislative bodies, are currently considering, it’s possible to predict customers’ equal and opposite reactions and, as a result, what the new normal could look like.

Photo by Nadine Shaabana on Unsplash
Action: Travelers who cross state or country borders must quarantine for 14-days unless they can prove that they are COVID-19 negative
Reaction: People will limit their travel to within their home states or countries
Most US states and many countries have 14-day mandatory quarantines in place for people traveling into their jurisdictions. Given that most trips last less than two weeks, these restrictions essentially make most travel impractical.
Some places, like Hong Kong and Vienna, are trying to lessen that barrier by testing arriving passengers at the airport and, if they test negative for COVID-19, exempting them from quarantine.
But until a vaccine is widely available, “travel is likely to return first to domestic markets with ‘staycations,’ then to a country’s nearest neighbors before expanding across regions, and then finally across continents to welcome the return of journeys to long-haul international destinations,” according to Cecilia Rodriguez, a senior contributor to Forbes.

Photo by Dino Reichmuth on Unsplash
Action: Prices increase due to fewer flights, reduced capacity
Reaction: Demand decreases as vacations become road trips and business travelers continue to use virtual meeting technology
According to research by Longwoods International, a research firm focused on the tourism industry, 82% of people traveling in the next 6 months have changed their travel plans. 22% of these people have changed from flying to driving. “Our clients are a little hesitant to get on an airplane right now,” Jessica Griscavage, director of marketing at McCabe World Travel in McLean, Virginia, told CNBC. “We’re already preparing for the drive market for the remainder of the year, and probably into 2021.”
In conversations I’ve had with business clients, the shift isn’t from air to road travel, the shift is more drastic – from traveling to not traveling. For most large companies, business hasn’t stopped or even slowed. Instead, it’s shifted to technologies like Zoom and Microsoft Teams. As people become more comfortable working “virtually,” these solutions will become far more attractive and just as effective as hopping on a plane.

Photo by CDC on Unsplash
Action: 4-hour pre-flight processing to ensure that all bags are sanitized, and all passengers are healthy
Reaction: Business travelers will choose private flights or fractional jet ownership over commercial air travel
The average business trip is approximately 3 days long according to Travel Leaders Corporate, an award-winning leader in business travel. With most days packed with meetings, executives will have neither the time nor the patience to devote half-a-day to check-in, security and health screening, and boarding.
Instead, they’ll opt for private or private-like offerings such as NetJets that offer an expedited check-in, screening, and boarding process.

Photo by JC Gellidon on Unsplash
Action: Longer flight turnarounds due to the need to sanitize planes
Reaction: Demand (and prices) for direct flights will increase while demand to get to places that don’t offer direct flights will decrease
Consultants often joke about the “Misery Tax” – the premium that clients in hard reach location have to pay to make it “worth the firm’s wile” to serve them. Although that may seem crass, there’s no debating that direct flights are significantly easier and less painful than ones that require connections.
The pain of connecting flights, however, is likely to go through the roof as the 30-minute turn-around times that airlines have been chasing become nearly impossible due to increased cleaning and sanitation guidelines. Gone will be the days when travelers worried about making their connections. Instead, they’ll worry about how to fill the hours between flights.
In fact, it’s likely that the misery of a given itinerary will shift from being a “tax” passed on to clients to a filter that business and leisure travelers will use when deciding where to travel.

Photo by Sharon McCutcheon on Unsplash
Action: Airlines will use the need for more screening and sanitizing to justify more fees
Reaction: People will fly only when needed, instead opting for other, cheaper, and easier convenient options.
With $82B in additional revenue from add-on fees, airlines aren’t going to pull back from charging for “extras.” Instead, the need for more passenger screening, social distancing, and control over what is allowed in the cabin, will inspire even more add-on fees.
For example, airline industry consulting firm, Simplifying, predicts that airlines will no longer allow passengers to pick their seats but will instead assign seats to ensure proper social distancing and offer passengers the opportunity to pay for premium seats and/or keep the seat next to them empty.
Other options under consideration are banning carry-on baggage (which conveniently increases the number of bags checked and therefore the revenue from checked-bag fees) and selling safety kits containing face masks, disposable gloves, and cleaning wipes.
Already tired of being nickel-and-dimed, travelers are unlikely to willingly pay extra for required services and, as a result, are more likely to be open to alternatives such as car trips or virtual face-to-face meetings.

Photo by JESHOOTS.COM on Unsplash
There will always be demand for air travel.
But it may take generations for demand to pre-COVID levels.
Unlike 2001 and 2008, air travelers have options beyond commercial air carriers. Wealthy and business travelers can opt for private jets or services offering fractional ownership. Businesses, already eager to cut costs, will be more open to virtual face-to-face meetings. Families can re-discover the adventure of road trips and the creativity of staycations.
It is the availability of these comparable options combined with the invisible threat of disease that will cause people to re-think their habits and default options and slow the airline industry’s recovery. If it ever fully recovers at all.
by Robyn Bolton | May 6, 2020 | Innovation, Stories & Examples
There is more to telemedicine – the exchange of medical information from one site to another through electronic communication to improve a patient’s health – than virtual visits with physicians.
Specialists like dentists, orthodontists, ophthalmologists, psychologists, and even veterinarians are using telemedicine solutions during the pandemic.
Like their physician counterparts, many resisted virtual visits until it became the only way to continue to care for patients and stay in business, as stay-at-home orders expanded from weeks to months.
Here’s a quick run-down of telemedicine’s use in other specialties and what the road ahead could look like for each.
DENTISTRY
Where we are now
According to the American Dental Association, since early March, 79% of dentistry practices closed except for emergency procedures, and another 18% closed completely.
This isn’t surprising given how COVID-19 is transmitted but, for patients in pain, it can be hard to know what constitutes a true emergency and what can be managed at home. Helping patients figure out what needs immediate attention and what can wait seems to be tele-dentistry’s sweet spot.
“Research indicates that 80% of acute dental concerns can be addressed at home without an in-person visit,” explains Chelsea Acosta Patel, Head of Wally Experience at Wally Health, a dental care start-up based in Boston. “Using technology, dentists can triage issues and care for patients while keeping them out of the chair.”
Where we go from here
The bigger, long-term opportunity, according to Patel, may be in preventative care by creating and monitoring at-home preventive care solutions across the patient dental journey.
“Most dentists don’t have the tools to keep an ongoing pulse with patients. They just assume that if a patient has an issue or a question, they’ll call the office. Teledentistry solutions enable dentists to develop customized, ongoing touchpoints to help patients remain healthy and catch potential issues early. This improves the patient’s experience, drives loyalty and word of mouth (pun intended) for the dentist, creating a virtuous oral health cycle.”
ORTHODONTICS
Where we are now
While Dentists need a way to answer questions, triage issues, and provide follow-up care, Orthodontists have a more pressing need – to make sure their patients’ jaws continue to develop and their teeth continue to move in the right way.
“We serve a vulnerable pediatric population whose jaws are developing. The adjustments we make as part of their treatment affect that growth and development,” explains Dr. Adam Welmerink of Welmerink Orthodontics in Reno Nevada. “When we realized this would be more than a 2-week shutdown, we needed a way to keep our patients safe, make sure their appliances weren’t doing any harm, and ensure their treatment was progressing as planned,”
Through services like Orthodontic Screening Kit (OSK), patients receive instructions on how to take photos and upload them to the OSK site for review by their orthodontists. Of course, the orthodontist’s ability to assess the patient’s need is determined by the quality of the photos, but, at a minimum, the service creates an opportunity for orthodontists to reconnect with their patients and give them guidance on signs that could trigger an in-office visit.
Where we go from here
Telemedicine in orthodontics, like many other specialties, will likely continue to be used to triage issues or to serve patients in remote rural areas.
“Many of our patients live in rural areas, with some driving 2 hours for a 10-minute appointment. We’ll probably continue to use (OSK) to see if they need to come in. And I could see using it in a limited capacity to triage patients who call with an emergency to assess if they can treat the issue at home or if they need to come in.” Dr. Welmerink mused. “Honestly, time-wise, it’s quicker to see a patient in the office. But this is great for right now.”
OPTHALMOLOGY & OPTOMETRTRY
Where we are now
Telemedicine’s use as a way to calm patients and triage concerns, deciding whether or not an in-office visit is required, continues with eye care.
“It is certainly a way to reassure patients that we are there for them, which is most important in these scary times,” NYC optometrist Dr. Susan Resnick told All About Vision.
While reassurance is important, most eye care professionals agree that telemedicine’s use is extremely limited. Proper eye care requires pupil dilation and specialized tools to accurately identify problems like glaucoma or assess the health of optic nerves and retinas.
Where we go from here
Despite its limitations, Dr. Resnick sees value in continuing to use telemedicine, “We will continue to utilize this platform whenever necessary. We do not view it as a disruptor or threat, but rather as a way to bolster our practice.”
Not everyone agrees.
“I’m not terribly enthusiastic (about remote eye exams),” Illinois ophthalmologist Dr. Benjamin Ticho told All About Vision. “There’s going to be too many mistakes. Plus, it diminishes the warmth and personality of the interaction. For many patients, a good doctor visit is a pleasant social occasion, and for many doctors, that’s part of why we went into medicine.”
MENTAL HEALTH
Where we are now
The data is staggering.
Before the crisis, 20% of US adults lived with mental illness but less than half received treatment according to federal statistics.
In the last two weeks of March, 45% of US adults felt that worry and stress related to COVID-19 were harming their mental health. It’s likely that number has increased as stay-at-home orders extend, and job losses and furloughs increase.
Yet the adoption of telemedicine to address mental health concerns has been slow. A phenomenon that is far from new. Case in point – over a decade ago, Congress excluded mental health providers from a $30M investment in digitizing patient health records. Even now, as CMS, private insurers, and state regulators are easing restrictions and increasing reimbursement for telemedicine to treat physical concerns, similar attention and flexibility have not been shown to mental health concerns.
As a result, “(providers) are kind of trying everything right now and seeing what can work,” John Torous, director of the digital psychiatry division at Beth Israel Deaconess Medical Center told Politico.
Where we go from here
More than other specialties, the jury is out on what happens next with regards to telemedicine for mental health.
On one hand, “so much of counseling has to do with body language, being physically present in the room, intonation,” Lynn Linde for the American Counseling Association told Politco. “Sometimes, that’s lost when you don’t have a good internet connection, or one of your starts getting garbled.”
On the other, this could be a “tipping point for the way we practice,” said Peter Yellowlees, a professor of clinical psychiatry at the University of California, Davis and former president of the American Telemedicine Association.
Optum, a division of UnitedHealth, seems to be betting on the latter. Last week it announced that it was in talks to acquire AbleTo, a New York-based virtual therapy provider for $470M, or 10x forward revenue.
VETERINARY CARE
Where we are now
If telemedicine is good enough for humans, it’s good enough for our animal companions.
A relatively new addition to the specialties offering telemedicine solutions, only a handful of companies are currently playing in this field. TeleVet, a “Texas-based, digitally optimized company focused on veterinary care,” is one.
Before the outbreak, TeleVet was in use in 1000 clinics across the US and even closed a $2M seed round in January.
“We can check for infections such as ear infections or drainage from either a still picture or a video, or even a live video conference with the owner,” Dr. Amy Garrou as Houston-area vet explained to Innovation Map. “The platform has been useful because we can do any of those consultations and get the information we need to manage the case without the pet owner having to come into the clinic.”
Where we go from here
Like dentistry, orthodontics, and eye care, telemedicine’s use in the Veterinary space is a boon for providers and patients at a time when it’s not safe to be in a crowded office. But as restrictions lift, like the other health care fields, it’s likely to be used primarily to answer questions, triage concerns, and perform post-surgery check-ups.
THE CLINICAL APPLICATIONS ARE DIFFERENT BUT THE ROAD AHEAD IS THE SAME.
Yes, telemedicine is an incredible tool to have in our collective healthcare toolkit. Its use across medical specialties is evidence that it fills a need for clinicians (provide care for my patients) and patients (address my concerns).
In “normal” times, those needs are well addressed by in-office visits, retail clinics, and urgent care. It is only in very specific circumstances, like when medical professionals cannot easily or safely see patients in-person, that existing solutions fall short and telemedicine becomes the most attractive option.
However, telemedicine only became an available option when regulators relaxed rules, insurers increased reimbursement, and patients accepted emails and video-chats as treatment.
It took a pandemic to create the confluence of circumstances required for physicians, dentists, orthodontists, eye care professionals, mental health caregivers, veterinarians, and other clinicians to begin or expand the use of telemedicine. It’s their experience, and the experiences and decisions of other players in the healthcare ecosystem, that will lead them back to the office and the hands-on care that is both desired and required.

by Robyn Bolton | Apr 28, 2020 | Customer Centricity, Innovation, Strategy
It was a large rectangular room. Chairs lined the walls. A children’s play area was tucked into a corner. One half of the room was labeled “Healthy Visits.” The other half was labeled “Sick Visits.” The check-in area was on the healthy side.
Even as a kid, this set-up made no sense to me.
Today, this set-up can be deadly.
That, along with stay-at-home orders and a myriad of other policies and practices, has propelled telemedicine to adoption and usage rates that companies like Teladoc, Doctor on Demand, and American Well could have only dreamed of 6 months ago.
But is this a new normal or will we go back to choosing a side of the large, open room in which to sit and wait?
Before we predict the path forward, let’s look at how we got here.
Telemedicine, according to the Centers for Medicare and Medicaid Services (CMS), generally refers to the exchange of medical information from one site to another through electronic communication to improve a patient’s health.
First commercially used in the mid-1960s by Massachusetts General Hospital to treat employees and travelers at Boston Logan International Airport[1], telemedicine as we know it today didn’t take shape until the early 2000s when high-speed internet access became more widely available.
Between Teladoc’s launch in 2005 and early 2020, adoption of the service was slow, stymied by insurance companies’ fears that easy access to physicians would increase visits without improving outcomes and therefore increase costs, medical boards’ implementation of guidelines governing how and with whom visits could occur, providers’ and patients’ beliefs that diagnosis and treatment require hands-on care, and, most importantly, lower reimbursement rates for telemedicine versus in-office visits.
Then COVID-19 happened.
- March 17: CMS announced it would:
- Reimburse office, hospital, and other visits furnished by telehealth to anyone, not just patients in rural communities, at the same rate as in-office visits
- No longer conduct audits to ensure that patients have a prior established relationship with the provider, previously defined as at least one in-person visit before using telehealth
- Waive penalties for HIPAA violations due to the use of unsecured technology, like FaceTime and Skype, assuming that health care providers were using the technologies in good faith to serve their patients
- April 3: FCC initiated $200M program, with funds coming from the CARES Act, to fund telehealth
Spurred on by these changes at the national level, throughout April, 47 state medical boards have moved to allow care to flow across state lines by waiving the requirement that the physician providing care via telemedicine channels must be licensed in the state where the patient is located at the time of treatment.
These changes created winners and losers.
With new federal and state guidelines in place, telemedicine took off.
- Cleveland Clinic went from 3400 visits per month to 60,000 in March
- NYU Langone Health went from 50 visits per day to 900 per day during the week of March 23
- Teladoc’s daily visits increased by 50% to 15,000 per day
- Austin Regional Clinic saw 50% of its visits shift to telemedicine
On April 3, Forrester released a report predicting that, by the end of the year, there would be 1B telemedicine visits compared to only 200M for general medical visits. (EDITORIAL NOTE: I don’t believe this projection one bit as it doesn’t pass the sniff test, but it is interesting in terms of highlighting the order of magnitude change that could occur)
But, as with every market shift, there are winners and losers.
Sadly, telemedicine’s gains seem to be coming at the expense of hospitals, community clinics, and rural patients.
According to data from Quandl, hospital revenues dropped as much as 55% since early February as “discretionary” visits have decreased 51% while ICU and OR visits decreased 34% and 59% respectively compared to Childbirth visits (used as a control in their analysis) which only decreased 6%.
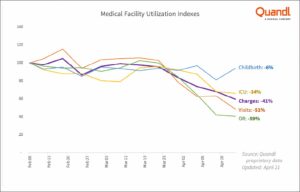
Source: Quandl proprietary data — revenue data from healthcare facilities nationwide.
Revenue and utilization decreases are hitting regional hospitals and community care centers especially hard.
Most impacted, however, seem to be rural areas where access to high-speed internet and laptops or phones with cameras are spotty at best.
“I practice in a somewhat rural area, as do many other doctors. So half of my patients are university types and have the technology. The other half are out driving tractors, or welding, or in construction. These patients often don’t have a video capability,” Dr. Christopher Adams, a rheumatologist at East Alabama Medical Center told AL.com. In fact, he estimates that 80-85% of his patients can’t do video appointments and he received only $12 in Medicare reimbursement for a 40-minute phone visit, the same rate as a 10-min in-office visit.
Echoing this disparity is Dr. Justin Cooke, a primary care physician and co-founder of Community Urgent Care, also in Alabama. “A lot of our Medicare patients don’t have the hardware or the knowhow to participate in a video chat format for a visit.” The result? An 80% decrease in revenue since the crisis started.
This won’t last forever.
To believe that “The demand has shifted forever on virtual care, and we’re on the verge of a new era for virtual care in the healthcare system,” as Teladoc CEO Jason Gorevic proclaimed in an interview with Jim Kramer on CNBC, you need to believe:
- CMS and other insurers will continue to reimburse all currently covered telemedicine at the same rate as in-office visits
- State medical boards will continue to allow patients to have visits with doctors they haven’t seen before and/or who practice in other states
- Doctors and patients will prefer the convenience of virtual visits to the personal, hands-on experience of in-office visits
I don’t believe a single one of those things.
When CMS changed its guidelines for telemedicine in mid-March, it added 85 services to its list of covered telemedicine services. With hospitals like the Cleveland Clinic and NYU Langone Hospital reporting that 75-80% of their telemedicine visits are with people who have a cough or worried they have COVID-19, it’s hard to believe that CMS’s list of covered services will stay as long as it currently is.
State medical boards have a vested interest in supporting their constituencies, the physicians operating in their states. With some health systems strained to the breaking point by COVID-19 and others managing excess capacity, allowing physicians to operate across state lines during the crisis simply made humanitarian and political sense. But with one-third of physicians in a survey conducted by Merritt Hawkins, a physician search company, indicating that they plan to change or close their practices as a result of the pandemic, state medical boards will be motivated to act fast to protect their members and their practices.
In terms of physicians, one could argue that the current 50% adoption rate, as reported in a survey by The Physicians Foundation, means that we’ve passed the tipping point. But it’s important to remember that the jump from 18% usage in 2018 to 50% today was akin to a forced-choice rather than a voluntary one and, as a result, may not stick when circumstances change.
Convenience is often cited as a reason for patients to adopt telemedicine and it’s hard to argue with the fact that a virtual visit is faster, cheaper, and easier than a trip to the doctors’ office. But convenience matters most when you’re engaging a transaction, a functional exchange of goods or services.
Most healthcare visits aren’t transactions. What drives physician and patient behavior has less to do with functional jobs to be done (logical, rational tangible problems to be solved or progress to be made) and more to do with emotional (how I want to feel) and social (how I want others to see me) jobs. In Jobs to be Done research that I have conducted with physicians and patients over the years, I have consistently heard that the most important and satisfying part of the care experience is the personal and physical connection. Physicians say that the most gratifying moments of their jobs are when their patients hug them or shake their hands to thank them for care while patients talk about how office visits are akin to visiting lifelong friends and having conversations with people who truly know, understand, and care about them.
I also don’t believe that telemedicine will snap back to the pre-COVID normal.
I believe that some changes, like allowing physicians to treat patients across state lines or with whom they don’t have a pre-existing relationship, will revert to pre-pandemic positions. Other changes, like CMS reimbursement levels, will change based on usage data and pressure from special interest groups.
I believe that in-person connections and relationships will continue to drive physician and patient preferences. As a result, telemedicine will continue to be a more convenient version of retail clinics and urgent care, something patients use when their Jobs to be Done are purely functional (e.g. fix me, stop the pain, make me feel better) and convenience is the highest priority.
I also believe that, with the expansion of CMS covered services, the biggest change we will see is greater use in the management of chronic disease. For many patients with chronic diseases like high blood pressure, high cholesterol, and even some auto-immune diseases, if their condition is properly controlled, the purpose of an office visit is to review test results and re-up prescriptions. All things that can be done more quickly, easily, and, yes, conveniently through telemedicine.
Yes, it certainly feels like we are in a “new era” of medicine.
But, when this is over, it will feel a lot more like a “new-ish” era, a variation on the theme of what came before.

by Robyn Bolton | Apr 20, 2020 | Innovation
“What happens next? You know, once all of this is over?” my friend asked. “There will be a new normal, but what will it look like?”
This is the question everyone is asking.
Lots of people proclaim to have the answer. Some are based on history, but history isn’t a great predictor of the future. Some opinions are based on trends and projections but rely assumptions which may or may not be true. Many are based on our hopes or fears, but those are grounded in emotions which can change from one moment to the next.
No one actually has the answer.
What we’re experiencing is a fundamental disruption to our way of life. It calls into question everything we believed to be true about ourselves and our worlds. It requires us to re-think things that we took to be inviolable truths. It is impossible to experience such a sudden and all-encompassing upheaval and emerge as if nothing happened.
We know things will be different once the restrictions (e.g. stay-at-home, limited gathering sizes, essential workers only, curfews) are lifted.
What we do not know is HOW they will be different and HOW LONG they will stay different.
I certainly don’t and that’s a terribly frustrating feeling. After all, I’m the person who reads the last page (or chapter) of a novel before I read the first because I want to know who is still alive and whether the ending is happy or sad. So, as you can imagine, I’m impatient to get at least a hint of what comes next.
Happily, there are ways to get that hint: Be curious, ask questions, seek input from a wide variety of sources, and observe how things progress.
Here are the questions I’m asking:
How will connection be different?
History says we’ll grow further apart. During pandemics, people choose, or are forced to, separate from one another, to stay at home, and to minimize contact with the outside world. Pandemics also highlight economic and social inequalities, disproportionately impacting the poor and working poor and inflaming class divisions. After the crisis passes, people remain wary of others and physically and emotional exhausted from the experience. They don’t want to re-live it by talking about it or, even worse, reflect on who they became during the experience.
OR…
We’re more connected than ever as the internet, social media, and video conferences make this a shared experience on a global scale. Yes, there’s a lot of crap on social media and Zoom-bombing isn’t helping things. But social media is also spreading good news — videos of people in Italy singing together and playing Bingo, people in various cities applauding healthcare workers, parades as substitutes for parties. Zoom, FaceTime, Google Hangouts, and similar services enable us to see the people we’re talking to, engage in the conversation (because it’s hard to multi-task on camera), and connect in deeper and more effective ways than we could by phone or email.
I HOPE that…
Connection takes on deeper meaning, that we’ll care more about the quality of our connections than the quantity and, as a result, invest more time with the people we care about than we do in generating likes and followers.
Gratitude continues to be part of our daily social interactions, that we say, and mean, “thank you” to the people working in healthcare, retail, restaurants, delivery, and other essential businesses.
Empathy remains a part of how we think and act because we have all shared an experience of great uncertainty, witnessed how fragile our lives and lifestyles are, and realized that we actually are all in this together.
How will work be done?
People will return to the office because they have grown tired of staying in their homes, relying on technology for virtual meetings, and having their calendars filled with meetings that were once hallway conversations. Offices are suddenly a welcome respite from the home because they are purpose-built for work, establishing physical definition between our work and personal selves, enabling direct human interactions, and creating an environment where connections between people and between ideas effortlessly occur.
Or…
More people will work from home because they value the flexibility and control it offers. Employers will have a hard time arguing that physical presence in the office is essential for most jobs when people have been working remotely for over a month. And those employers that do mandate a return to the physical workplace risk sending the message that they don’t trust their employees which could, in turn, result in employees leaving for a different employer that does trust and respect them as adults.
I PREDICT that…
Employers and employees will work together to figure out what works best. Old school managers who once resisted letting people work from home for fear that no work would be done are experiencing the reality that people are as, or more, productive at home than in the office. While employees who clamored to work from home now miss the informal chats, hallway conversations, and sense of community that are part of working from an office.
How will learning and education occur?
School will look like it did pre-COVID-19. Kids want to be back with their friends and parents don’t want to be teachers, principals, hall monitors, and test proctors. As a result, kids will go to a school building, sit in a classroom with other students their age, and teachers will teach what the curriculum requires. Inequity will continue as the richest schools are able to attract the best teachers and the most and latest resources, while the poorest schools will scrap by, focused as much (if not more) on meeting basic needs, like food, clothing, and cleanliness, as they do on teaching reading, writing, and arithmetic.
Or…
School is no longer a physical place but a set of activities and interactions. Learning happens when and how best for the student (within certain parameters, of course) and parents stay engaged in what, how, and when their kids are learning. Teachers will continue to find new ways to teach, including recording lessons once taught live to a full classroom and then engaging live with students one-on-one. Everyone will have more freedom to explore, create, discover, socialize, and learn.
I HOPE that…
This seismic shift in what it means to go to school will open people’s minds to what’s possible and increase their willingness to experiment as a means to reduce inequity and raise what’s “minimally acceptable.”
But I PREDICT that…
There will be innovation on the margins, that those who have the most resources will enjoy most of the benefits, and the majority will return to the pre-COVID-19 status-quo.
HOW LONG will the “new normal” last?
We’re human and we don’t like change. We especially dislike change when it’s forced on us. Even in the best of times, we want safety and security and we crave those things even more in periods of uncertainty. As a result, we will go back to the “old normal” as soon as we possibly can.
Or…
We have been fundamentally changed and therefore lasting change is inevitable. We see how hard healthcare workers work and the sacrifices they make. Parents are experiencing how hard teachers work and, if the tweets are to be believed, are willing to pay them millions to resume their roles. We appreciate the essential workers working grocery stores, delivering packages, and maintaining our infrastructure. We’ve returned to having conversations with family members, cooking and eating meals together, and reaching out to people who matter the most. We’ve been forced into a “new normal” but, by the end of it, it will simply be “normal.”
I PREDICT that…
The duration of the “new normal” depends entirely on how long the current situation lasts. The longer this situation — social distancing, stay at home orders, schools and non-essential businesses closed, the numbers of the sick and the dead leading the news — the greater the likelihood that things that felt new and different two weeks ago will become normal habits and expectations that endure. But, if the worst truly is over by April 30 and there’s no Round 2 in the summer or fall, we’ll return to the “old normal” as soon as we possibly can.
Originally published at https://www.datadriveninvestor.com on April 20, 2020.
