Isaac Newton Knows What’s Next for Air Travel
I took my last flight on Friday, March 13, two days after the president’s first address to the nation about COVID-19.
It was a JetBlue flight from Charlotte, NC back home to Boston. And it was awesome!
Setting aside the fact that I was wearing disposable gloves and wiping down every surface with Clorox wipes, I felt like I was flying private. I was the only person in my row, with no one in the row ahead of or behind me. Snacks and drinks were plentiful. The stewards were friendly and attentive. Even the boarding process was swift and orderly.
But when stay-at-home orders went into effect the following Monday and I shared my travel story with clients, they were aghast. How could I take such risks? Did I feel safe? Did I wear a mask?
Their reactions surprised me. After all, these executives are frequent travelers, even road warriors they travel so much. Yet the fear in their voices revealed a changing perception of travel. What was once a necessary evil for work and an efficient solution for vacation had, in just 3 days, become a senseless risk.
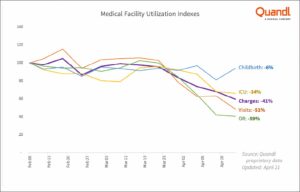
In the 2 months since that flight, the airline industry has been rocked. Consider:
- 94% drop in US commercial airlines’ passenger volume
- 80% decrease in US private jet flights
- 75% decrease in the number of worldwide commercial flights per day
- 80% decline in the global daily number of flight searches
- 61% increase in the amount of time between booking and traveling
That last stat – 61% increase in the amount of time between booking and traveling – indicates that people don’t expect to fly any time soon. But is that expectation a reaction to the drastic measures taken to flatten the curve or is it a sign of changing travel habits?
Many experts and industry associations are looking to data about the airline industry’s recovery post-9/11 and the 2008 global financial crisis. According to data from Airlines for America, it took 3 years for passenger volume and revenue to return to pre-9/11 levels and approximately 7 years to recover to pre-2008 financial crisis levels.
Here’s the harsh truth – we cannot possibly know what will happen next. 9/11 and the 2008 financial crisis were fundamentally different events than what we’re experiencing now.
So while I understand why people are looking to these past events – data offers a sense of comfort and control over the future – using data from them is pointless. It offers a warm snuggly illusion that things won’t change that much and a return to the old days is inevitable.
Instead of looking to the past for answers, we need to look to physics.
Newton’s 3rd Law, to be precise. It states that for every action, there is an equal and opposite reaction.
By looking at the actions that airlines, and regulatory and legislative bodies, are currently considering, it’s possible to predict customers’ equal and opposite reactions and, as a result, what the new normal could look like.
Action: Travelers who cross state or country borders must quarantine for 14-days unless they can prove that they are COVID-19 negative
Reaction: People will limit their travel to within their home states or countries
Most US states and many countries have 14-day mandatory quarantines in place for people traveling into their jurisdictions. Given that most trips last less than two weeks, these restrictions essentially make most travel impractical.
Some places, like Hong Kong and Vienna, are trying to lessen that barrier by testing arriving passengers at the airport and, if they test negative for COVID-19, exempting them from quarantine.
But until a vaccine is widely available, “travel is likely to return first to domestic markets with ‘staycations,’ then to a country’s nearest neighbors before expanding across regions, and then finally across continents to welcome the return of journeys to long-haul international destinations,” according to Cecilia Rodriguez, a senior contributor to Forbes.
Action: Prices increase due to fewer flights, reduced capacity
Reaction: Demand decreases as vacations become road trips and business travelers continue to use virtual meeting technology
According to research by Longwoods International, a research firm focused on the tourism industry, 82% of people traveling in the next 6 months have changed their travel plans. 22% of these people have changed from flying to driving. “Our clients are a little hesitant to get on an airplane right now,” Jessica Griscavage, director of marketing at McCabe World Travel in McLean, Virginia, told CNBC. “We’re already preparing for the drive market for the remainder of the year, and probably into 2021.”
In conversations I’ve had with business clients, the shift isn’t from air to road travel, the shift is more drastic – from traveling to not traveling. For most large companies, business hasn’t stopped or even slowed. Instead, it’s shifted to technologies like Zoom and Microsoft Teams. As people become more comfortable working “virtually,” these solutions will become far more attractive and just as effective as hopping on a plane.
Action: 4-hour pre-flight processing to ensure that all bags are sanitized, and all passengers are healthy
Reaction: Business travelers will choose private flights or fractional jet ownership over commercial air travel
The average business trip is approximately 3 days long according to Travel Leaders Corporate, an award-winning leader in business travel. With most days packed with meetings, executives will have neither the time nor the patience to devote half-a-day to check-in, security and health screening, and boarding.
Instead, they’ll opt for private or private-like offerings such as NetJets that offer an expedited check-in, screening, and boarding process.
Action: Longer flight turnarounds due to the need to sanitize planes
Reaction: Demand (and prices) for direct flights will increase while demand to get to places that don’t offer direct flights will decrease
Consultants often joke about the “Misery Tax” – the premium that clients in hard reach location have to pay to make it “worth the firm’s wile” to serve them. Although that may seem crass, there’s no debating that direct flights are significantly easier and less painful than ones that require connections.
The pain of connecting flights, however, is likely to go through the roof as the 30-minute turn-around times that airlines have been chasing become nearly impossible due to increased cleaning and sanitation guidelines. Gone will be the days when travelers worried about making their connections. Instead, they’ll worry about how to fill the hours between flights.
In fact, it’s likely that the misery of a given itinerary will shift from being a “tax” passed on to clients to a filter that business and leisure travelers will use when deciding where to travel.
Action: Airlines will use the need for more screening and sanitizing to justify more fees
Reaction: People will fly only when needed, instead opting for other, cheaper, and easier convenient options.
With $82B in additional revenue from add-on fees, airlines aren’t going to pull back from charging for “extras.” Instead, the need for more passenger screening, social distancing, and control over what is allowed in the cabin, will inspire even more add-on fees.
For example, airline industry consulting firm, Simplifying, predicts that airlines will no longer allow passengers to pick their seats but will instead assign seats to ensure proper social distancing and offer passengers the opportunity to pay for premium seats and/or keep the seat next to them empty.
Other options under consideration are banning carry-on baggage (which conveniently increases the number of bags checked and therefore the revenue from checked-bag fees) and selling safety kits containing face masks, disposable gloves, and cleaning wipes.
Already tired of being nickel-and-dimed, travelers are unlikely to willingly pay extra for required services and, as a result, are more likely to be open to alternatives such as car trips or virtual face-to-face meetings.
There will always be demand for air travel.
But it may take generations for demand to pre-COVID levels.
Unlike 2001 and 2008, air travelers have options beyond commercial air carriers. Wealthy and business travelers can opt for private jets or services offering fractional ownership. Businesses, already eager to cut costs, will be more open to virtual face-to-face meetings. Families can re-discover the adventure of road trips and the creativity of staycations.
It is the availability of these comparable options combined with the invisible threat of disease that will cause people to re-think their habits and default options and slow the airline industry’s recovery. If it ever fully recovers at all.